





万思泰科技致力于打造全新柔性快响应生产解决方案,服务多品种小批量制造企业,助力制造行业转型升级。我们通过深度融合人工智能与机器人技术,实现AI驱动的生产全流程柔性化和智能化,帮助客户在效率、质量与可持续性上全面领先。
我们通过工艺创新、流程优化、设备智能化、产线重构,系统性地提升生产的效率,保证产品质量,为制造企业客户提供快速交付的能力。
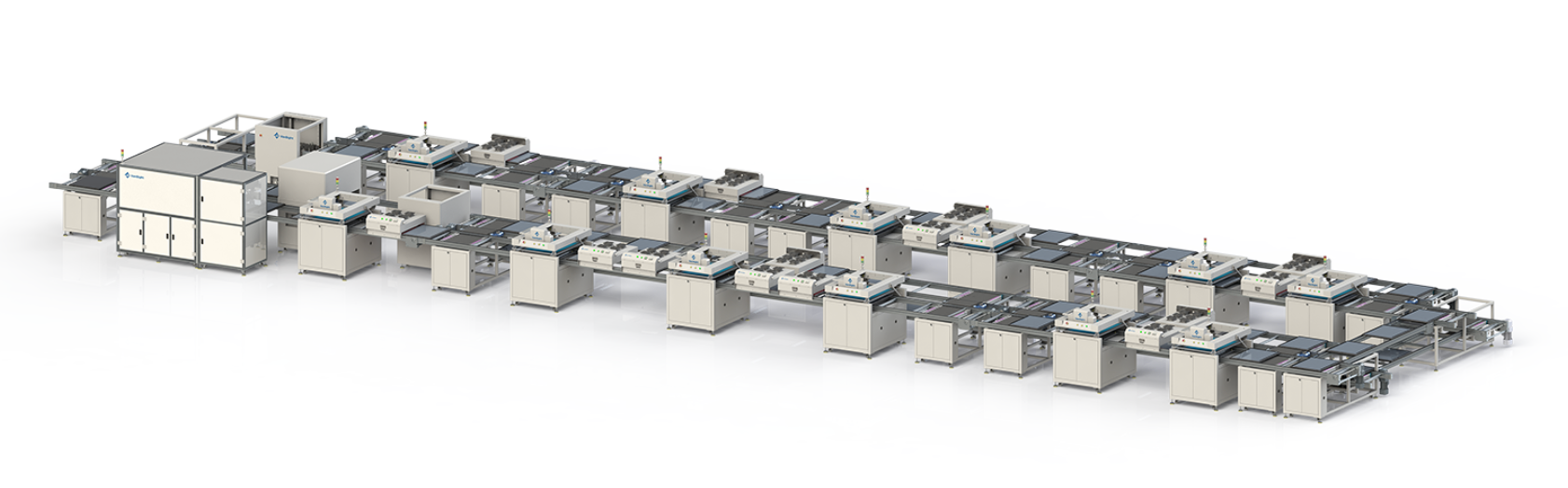
我们以AI驱动产线自适应,分钟级切换生产款式,让每一台设备都能精准响应消费者的个性化需求,让产能与需求无缝对接。
为了减少我们的碳足迹,将生产搬到离消费者更近的地方是必然的选择。可持续性是我们基因中的一部分,也是应对未来挑战的回答。
通过自动化、数字化、智能化技术和精益化理念,我们能够提供更高质量、更好体验的产品,使用客户在国际竞争中持续保持竞争力。
Vansight Group
北京地址:北京市 海淀区 彩和坊路10号 1+1大厦 612
福建地址:福建省 晋江市 陈埭镇 江头 前进路南163号
邮箱: admin@vansight.net
电话:18600752528
© 2026 万思泰 VanSight
隐私政策